Table Of Content
- Basic principle, model assumptions, estimator of treatment effect
- Stepped Wedge Cluster Randomized Trials: A Methodological Overview
- TRESemmé TRES Two Mega Firm Control Gel
- Stepped Wedge Randomized Controlled Trials
- Epidemiology and study details
- Stepped Wedge Cluster Randomized Designs for Disease Prevention Research
The stepped wedge trial has other advantages over parallel cluster designs of a technical nature, but it also has disadvantages. In the rest of this paper we discuss these statistical and technical features and identify situations where this design is more or less suitable than alternatives. Challenges of the SW-CRT design included (1) time-sensitive recruitment, (2) retention, (3) randomization requirements as opposed to practice preferences, (4) achieving treatment schedule fidelity, (5) intensive data collection, (6) the Hawthorne effect, and (7) temporal trends. An SWT is a trial in which clusters receive the intervention at different time points, the order in which they receive it is randomised, and data are collected from clusters over time. The stepped-wedge design (SWD) of clinical trials has become very popular in recent years, particularly in health services research.
Basic principle, model assumptions, estimator of treatment effect
Consequently, there is limited published guidance for planning SWTs, and adapting the published guidance to the broad range of designs in use is not straightforward. The studies varied considerably in terms of number of steps and number of participants (Table (Table3).3). In two of these studies [14,17] participants are randomised to two cohorts, with one cohort receiving the intervention while the other cohort served as the control. In addition to the conventional flow diagram, we recommend that a design diagram should illustrate how many participants are within each cell of the design.
Stepped Wedge Cluster Randomized Trials: A Methodological Overview
However, the stepped wedge design requires a longer trial duration than parallel designs and also presents a number of challenges, including both practical and statistical complexity. Hence careful planning and monitoring are required in order to ensure that a robust evaluation is undertaken. In a continuous recruitment short exposure design stratification and restricted randomisation could be based on characteristics of clusters, or of historical cluster summary values of outcomes or other characteristics of individuals within clusters. In a closed cohort design, besides this information, it may be possible to use cluster summary values of the characteristics of individuals who will participate in the trial if these are known before randomisation. In an open cohort design it may likewise be possible to use information from individuals who will participate at the start of the trial. Two common problems faced by CRTs are imbalance in important characteristics across study arms despite randomising the clusters (particularly where the number of clusters randomised is small), and substantial reductions in power resulting from between-cluster variation.
TRESemmé TRES Two Mega Firm Control Gel
The published protocol does not state whether patients may participate more than once in the trial, nor exactly what might happen to patients presenting just before a hospital changes to the intervention condition. However, as the exposure of the patient primarily relates to their management within the first few hours of arrival at hospital, it would seem that nearly all participants will be exposed to the control or intervention condition, and not both. Like other cluster randomised trials (CRTs), SWTs are generally designed to study the effects of a new intervention, such as a policy or staff training programme which is implemented at the cluster level, but experienced and measured by its impact on individuals. For example, in a situation where hospital staff implement a new patient management policy, the SWT is designed to establish whether this leads to better outcomes for patients who are treated at the hospital. When planning an SWD, it is important to realize that the procedure to be used for calculating power cannot be converted into a simple formula for the number n of clusters that start the intervention at the same time. Est, as well as the power, depend not only on the variance (s²) of the cluster means and the number of clusters (n), but also on the number of intervention start times (T) and the correlation between repeated measurements in a single cluster.
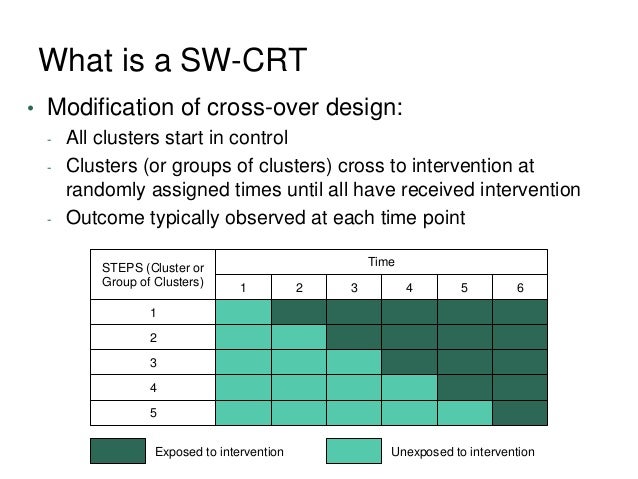
A typical feature of SW-CRTs is that all clusters will eventually be exposed to the intervention during the study period. Figure 1 provided an illustration of a SW-CRT with the Early Recognition and Response to Increases in Surgical Site Infection (Early 2RIS) Trial.8 Thirteen surgical procedures were classified into six types (e.g., cardiac, spine, etc). Clusters, constructed at each of the 29 study hospitals based on the type of surgical procedure performed, were the units for randomization and analysis. The study randomized 105 clusters over 14 periods to assess the effectiveness of surveillance using optimized statistical process control methods and feedback on rates of surgical site infections compared to traditional infection surveillance methods. In Figure 1, there are 12 randomization sequences; each randomization sequence is determined by the first period a group of clusters crossover from control to intervention. This is in comparison to parallel-arm designs, where usually half of clusters are simultaneously randomized to either intervention or control at baseline.

Second, there may be logistical, practical or financial constraints that mean the intervention can only be implemented in stages [3]. In such circumstances, determining the order in which participants receive the intervention at random is likely to be both morally and politically acceptable and may also be beneficial for trial recruitment [7]. An example of an intervention where a stepped wedge design may be appropriate in evaluation is a school-based anti-smoking campaign that is delivered by one team of facilitators who travel to each participating school in turn. One limitation of our review is the possibility that our search strategy did not identify all of the studies that have employed a stepped wedge design. In particular, we may have missed 'delayed intervention' studies with two steps, in which the delayed group receive the intervention after the outcomes from initial intervention group have been evaluated, but where the outcomes of the delayed group are also evaluated. We have included three studies of this nature in this review [12, 14, 17] although it is questionable whether studies with only two steps should be considered as stepped wedge designs.
Emphasis is on application, with examples in disease prevention and health promotion research. Carry-over effects are widely discussed in the literature on individually randomised crossover trials [22]. This design is commonly used with individuals with a chronic condition who are randomised to receiving a standard treatment for a certain period followed by a new treatment, or vice versa. Health is measured during each period to determine which treatment is better, and there may be a ‘wash-out’ period between the two treatments so that there will be no carry-over effect of the first treatment during the second period. Carry-over effects are always considered, and can arise if the new treatment has a permanent effect on the health of participants after a short period of administration. 2 of their paper, Hemming et al. describes a design where data are obtained from each cluster in the step before the crossover and for two steps afterwards [3].
This creates burdens on practices not being able to choose when to start the intervention and on the study team to retain sites while they wait to receive the intervention. It is also possible that the perceived value of participating in the study is discounted over time, resulting in practices dropping out. He provides a general model representation and regard various model extensions as alternative ways to characterize the secular trend, intervention effect, and sources of heterogeneity.
How to describe exposure and measurement in a stepped wedge cluster randomised trial
The first reason is that these data do not directly inform the estimation of the intervention effect unless strong assumptions are made concerning period effects before during and after the rollout period, which is inadvisable. Without such strong assumptions the gain in precision is modest, arising from information concerning variability between clusters. The second reason is that including these data may introduce bias unless the model for these data over the data collection period is correctly specified, which is more difficult to do as the period becomes longer. Collecting data well after the rollout period may, however, be worthwhile if a secondary analysis of whether the intervention effect appears to be sustained is very important. Poldervaart et al. are conducting a trial to investigate the effect of introducing a policy promoting the use of a scoring system to guide clinical decisions for patients with acute chest pain on arrival at hospital emergency departments [9].
Cooperatives that deviated from using SW-CRT design did so to mitigate logistical challenges. Even if the cluster means obtained in an SWD trial are normally distributed, approximations are usually needed to test hypotheses concerning the treatment effect. They yield different results, and none can be said to be generally preferable to the others. Furthermore, as is often the case when analyzing longitudinal data, SWD trials are usually analyzed on the basis of assumptions about the correlation structure that greatly simplify the true situation (equicorrelation model). These include the treatment effect, the number of time periods, the number of groups, the number of members per group, ICC, CAC, IAC, and the correlation decay structure.
It also wicks away moisture, molds to the shape of your feet and is lightweight but durable. Unlike some of our other picks, the Brooklyn Low Wedge is soft and doesn’t require any breaking in (if you’re ever worn a pair of Crocs you’re familiar with the instant comfort). The lower wedge still adds a little height and the adjustable heel strap—with a cool, minimal pushpin-style closure—adds stability as you move. The EVA footbed is molded to the foot’s shape and like all Vionic shoes, they’re biomechanically engineered to provide arch support, stability and flexible cushioning. For some, the orthotic support might initially feel different, so the brand recommends wearing them for a couple hours a day until you’re fully used to them. Multiple reviewers also say these have a narrow fit, so consider the wide sizing if you’re in between widths.
In order to get the research done, the researcher must be alive to the concerns of other stakeholders. The SW-CRT design allows resources to be allocated over a longer period, a key advantage for large-scale implementations for which there might be limited resources. Owing to the staggered intervention start and end dates, resources, including the implementation team, can be shifted from one sequence to another, which eases workforce logistical concerns. In comparison, activities of parallel CRTs are condensed into a short time frame and are thus more resource intense. To identify the advantages and challenges of using SW-CRT design, we used the rapid assessment process, an “intensive, team-based qualitative inquiry using triangulation, iterative data analysis, and additional data collection.”21 We conducted semistructured interviews with all 8 grantees. We sent an e-mail invitation to the principal investigators and encouraged them to invite relevant team members (purposive snowball sampling22); all grantee principal investigators agreed to participate, with some electing to be interviewed alone, and others inviting up to 2 team members to join.
An example of the logistics of a stepped wedge trial design is shown in Figure 1, which shows a stepped wedge design with five steps. Data analysis to determine the overall effectiveness of the intervention subsequently involves comparison of the data points in the control section of the wedge with those in the intervention section. An example of the logistics of a stepped wedge trial design is shown in Figure Figure1,1, which shows a stepped wedge design with five steps. No two studies use the same methods of analysing data, although most compare outcomes in the intervention and control sections of the stepped wedge across the entire data set. These methods vary considerably in terms of their complexity and there is insufficient information to determine the appropriateness of each method. The two studies that apply step-by-step analysis [4, 13] provide a separate analysis for each step in the trial, in order to separate out underlying time trends.
Comparison of statistical models for estimating intervention effects based on time-to-recurrent-event in stepped wedge ... - BMC Medical Research Methodology
Comparison of statistical models for estimating intervention effects based on time-to-recurrent-event in stepped wedge ....
Posted: Tue, 26 Apr 2022 07:00:00 GMT [source]
Further work in this area might address other approaches to restricting the burden of measurement, for example collecting data from all clusters at all measurement times but varying the proportions of participants measured, so that measurement is unbalanced across clusters. This sampling option would increase the power from a ‘vertical’ analysis of the data [14]. With this design, a substantial number of individuals are identified and participate from the start, but some may leave during the trial and others may become eligible and be exposed for some time. Most participants will be exposed to both control and intervention conditions during the trial. Repeated measurements from the same individuals could be taken at times relating to their individual start of exposure, or researchers may choose to use a time-to-event outcome. However, these choices may be problematic in some trials due to individuals leaving the cohort over time, resulting in missing data.
Finally, we reviewed and discussed the matrix at multiple meetings to determine themes as advantages or challenges of SW-CRT design. Results were shared with grantees for participant checking and feedback; grantees confirmed that their perspectives were captured accurately and completely. Alternatively, an SWD trial can also be regarded as a sequence of T + 1 parallel-group trials, with a constant sample size (n) but a proportion of observational units allocated to the invention arm that varies over time (increasing from 0 to 100%).
He reviews the key model ingredients and clarify their implications for the design and analysis of such trials. This talk may serve as an entry point to understanding the evolving statistical literatures on stepped wedge designs. The issue of carry-over effects seems to have received very little attention in the literature on the SWT design, because the crossover is always from control to intervention, and so the obvious reasons to consider carry-over effects described earlier do not apply.








No comments:
Post a Comment